Information for lower limb amputees & their families

What to expect before, during and after amputation surgery
The most important goal of your entire treatment from the operation to rehabilitation, to the fitting of your prosthesis is to restore your mobility.
Your rehabilitation team, which includes your doctors, therapists, prosthetists and of course, you and your loved ones, will help you achieve the most independence possible, so that you can lead an active and mobile life. On average, this rehabilitation process takes between two to six months, although this can be affected by various factors, including your level of motivation and how well your prosthesis fits.
Recommendations with regard to your therapy and rehabilitation are provided below. However, the instructions from your rehabilitation team always take priority since this team is best able to evaluate your individual situation.
Before Amputation
Whether you’ve known about your amputation surgery for a while, or just found out, remember that you’re not alone. Your treatment team is there to support you, answer questions—and find the best solutions for you.
Initial Examinations
If you are to undergo planned amputation surgery, you will be examined in detail several times before the surgery. Your doctors will explain what will happen both during and after the operation.
During these discussions, you have the opportunity to ask any questions which are important to you. It’s a good idea to take notes of what you want to ask the doctor before the discussions so that you don't forget anything. Remember that it’s their job to explain it all clearly to you.






Amputation





After Amputation
Immediately after the operation, the focus will be on your recovery and the healing of your residual limb. Both are important so that you can start rehabilitation soon and be fitted with a prosthesis.
What should you expect after an amputation?
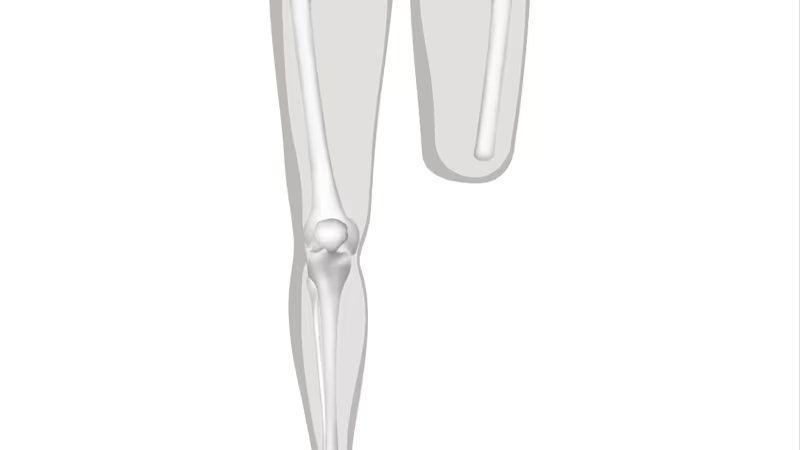
After the amputation your residual limb will be treated with a special wound healing bandage. Your doctor's main goal here is to quickly heal the wound that was caused by the operation and to prepare your residual limb for your future prosthesis.
The focus during the initial period after the operation is on three treatment goals: You should have little to no pain, your residual limb should be able to bear weight, and you should be able to move your residual limb optimally in all directions.
In order for all of this to succeed, it is important for you to have your doctor or physical therapist show you a few important things right after the operation. This includes correct positioning in bed so that the muscles and the joint adjacent to the residual limb don't retract or become stiff, as well as regular exercise. These measures allow you to be fitted more quickly and easily with a prosthesis so that you can remain mobile and active.


















Fitting and Rehabilitation
The Rehabilitation Process
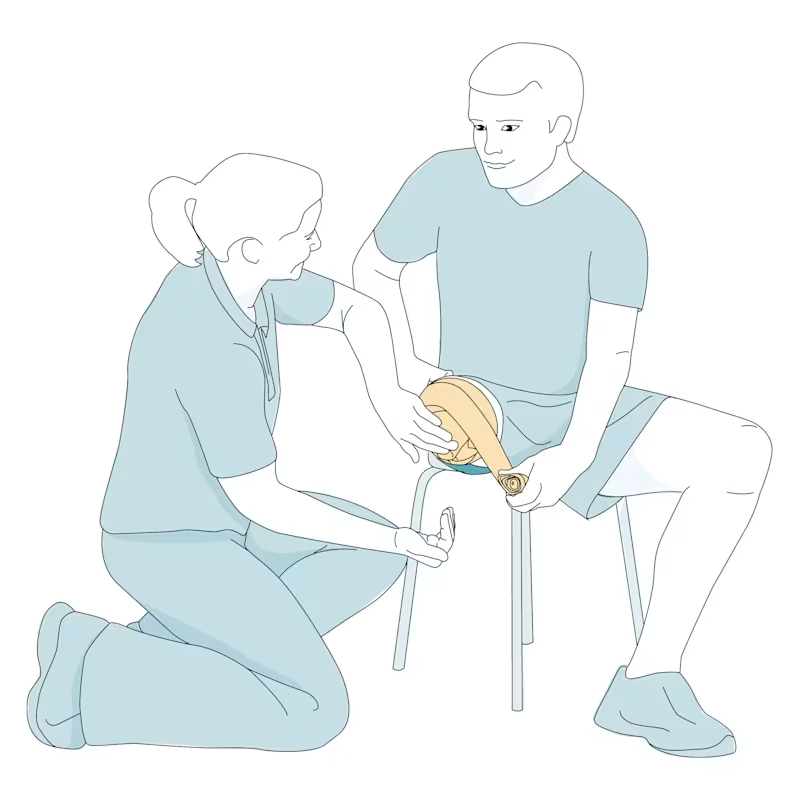
Your treatment team will decide when you can start with intensive rehabilitation based on how your recovery is going. During your rehabilitation process, you’ll be fit with a prosthesis tailored to your specific needs, and supported by a rehabilitation team that could include doctors, physical and occupational therapists, a prosthetist and nursing staff. These professionals are there to support you and to ensure that you are well prepared. During rehabilitation you will learn how to properly care for your residual limb, as well as the rest of your body.
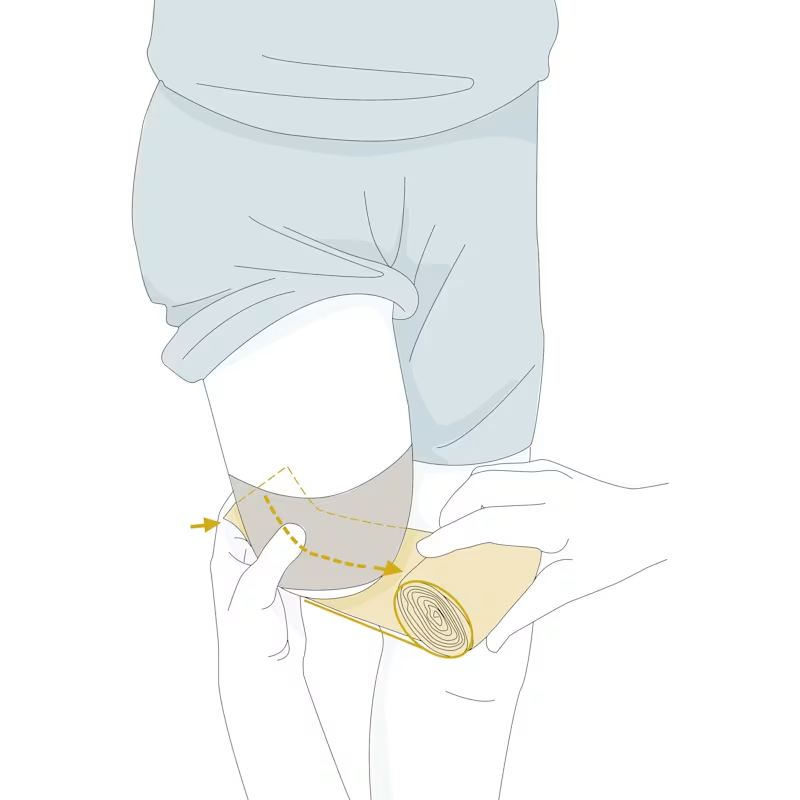
Before you can wear a prosthesis, your residual limb must be healed and have attained the proper shape. This means that all fluids that accumulated due to the operation have been removed through compression therapy and that the residual limb edema has subsided.
Once your residual limb has been properly formed and can bear weight, you may be fitted with an early or interim prosthesis. Then you’ll begin to practice using your prosthetic leg. At first you’ll learn how to put the prosthesis on and take it off as well as take care of it. Later, you’ll learn how to walk with the prosthesis, which is known as gait training.













